

This is the part 8 of a series that should be read in order.
Key Points:
- Asymmetrical RCSP need asymmetrical corrections (if we can)
- Case Presentation of Asymmetrical Pronation and Initial Measurements and Treatment
- Comments on Kirby Skives and Heel Structure and Tolerance
I want to start our discussion today on a patient I am just starting to treat. She presented with bilateral ankle pain. She was a runner who had been off for awhile and just starting back in old shoes and old orthotic devices. She came in to get new orthoses. Her pain was more lateral on the right ankle and more medial on the left ankle.

When I watched her walk, and run, in her old shoes, and then later with her new shoes, the same pattern occurred. Pronation was present bilaterally, but worse on the left, and some shift laterally (supination tendency) at times on her right. The image is of her standing. Even though I am just beginning to work her up, I will share biomechanical data so far collected. Often in private practice you have to consistently collect more and more data each time that you see the patient. The first question is; what is making her left side more pronated? She is right handed, and her left side is her support side, and therefore should be her most stable side. First of all, she mentioned the left side is the longer leg, but I have not measured that yet. Look at the data below I did collect noting why she pronated so much on that left side. I propose that the Forefoot Varus could be a Forefoot Supinatus and the MPE is functional also.
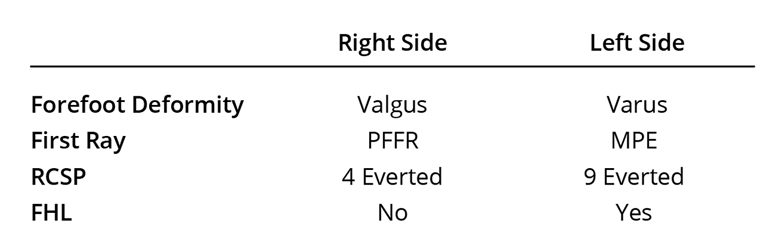
During gait analysis, it was the same pattern with limb dominance to the left side (landing harder and her trunk more over the left side). Remember also, 1/16 inch is 1 degree difference in RCSP, so these asymmetrical measurements are indicative of a 5/16 inch functional left short leg if she has no structural short leg that she was compensating by pronating more on this left side (to be measured later). In cases like this, and so many others with asymmetrical presentation, you have to decide the order of correcting things. Here I chose, in my mind, making a dent in the pronation problem, then adding lifts if a short leg is found (usually at the 2-3 month level), and also adding PT to assist with muscle balancing (usually earlier on after orthotic dispense).
I can not wait to look at limb length and muscle strength and OCSP. I am starting with just attempting vertical heel correction (getting her heels to vertical) and not NCSP (which will be measured at the next visit), since the left is so severe, more than twice as pronated as the right. I will be dispensing orthotic devices before this post is published, so after that visit I will add more to her exam.
Right Foot needs 4 degrees to Vertical (my initial Goal here): Here is what I have previously taught.
P1 is your B orthotic device with 3-4 degrees of extra pronation correction.This is accomplished many ways within the industry. P2 is a combination of these four variables to obtain an increase to 5-6 degrees of pronation correction. What methods are utilized for 3-4 degrees of additional heel correction?
- 4 mm medial heel (Kirby) skive
- 4 degree intrinsic varus cant (called “pour”)
- 4 degrees extrinsic varus rearfoot and forefoot posting
- 15-20 Degree Inverted Orthotic Technique
I am actually starting with option D at 20 degrees Inverted pour.
Left Foot needs 9 degrees (with 7 degrees my highest starting point) to get to heel verticality: Here is also what I have previously taught.
P4 is a 35 degree Inverted device or 25 degree with 2-3 mm medial Kirby skive. Here you are attempting 7-8 overall degrees of correction, which is also my personal maximum starting point in orthotic corrections that I will give to a patient. After making thousands of these P4 devices, not only do they accomplish what I am proposing, but they are very comfortable whenever the patient needs this correction. I have talked to many skilled clinicians that can accomplish the 7-8 degrees of correction with 15 degrees of Inversion, 3 mm medial Kirby skive, and 2 degrees of varus extrinsic forefoot and rearfoot posting.
I am actually starting P4 at 35 degree Inverted.
From our previous posts, the right side FF Valgus could be corrected with ASIS, but I prefer 20 degrees of the Inverted Technique to give me 4 degrees inversion (since it is being used on the left side). Since the left is FF varus, I could support up to five degrees intrinsically (giving around 2 plus degrees of heel change), add a 4 mm medial Kirby (giving me 2 degrees more), and then add a 3 degree extrinsic varus anterior and posterior posting (for a total of 7 degrees). It is easier for me to get the 7 degrees (my maximum starting point to see how a patient responds) with a 35 degree Inverted device.
Whether you use Kirby Skives or Inverted Technique, complaints of arch irritation are really rare, even though the arch height is nice and high. Why? Simple physics. You are placing the majority of the pronation correction at the heel which we take the highest pressure (and take the stress off the softer arch issue and avoid potentially blocking first metatarsal plantarflexion).
As you know by looking at feet all the time, heels come in all different shapes. Kirby heel skives, as the name suggests, requires that some of the original heel be removed. Some heels are too small for even 4 mm skives. And, the transition from heel to arch has to be smooth and gradual.
I personally love the Kirby skive, but I never use a flat plane which tends to have a 50% intolerance in my hands by the patients. I love to take away the medial side of the heel while rounding and blending! I want to get this correction on the medial side of the subtalar joint axis as Dr. Kirby has instructed. When doctors, labs, or new lab technicians or scanning software, are learning the technique, much like the Inverted Technique, analyze the patient's reaction. If there are complaints, ask what seems to be happening? It took Root Laboratory 2-3 years to get the arch height consistent while we were learning. Using either technique, the flatter the heel in the scan or cast, the more powerful the correction. Rounder heels sometimes just stay round as you invert or Skive and do not actually lift up that much in the medial heel area off the supporting surface.
Review of all the Orthotic Types Being Presented
Corrective Orthotic Devices
↓
- Balancing (B): (B1 and B2)
- Pronators (P): BP, P1, P2, P3, P4, P5, and P6
- Supinators (S): BS, S1, S2, S3
- M/L Instability (M): BML, ML1, ML2, ML3, ML4, ML5, and ML6
- Shock Absorption (C): BC, C1/C2, C3/C4/C5, C6, and C7
- Sagittal Plane (H): BH, H1, H2, and H3


